Brigham Young University–Hawaii (BYU-Hawaii) is a private undergraduate co-educational university in the United States. The University is affiliated with the LDS Church and is named after religious leader and politician Brigham Young.
Brigham Young University–Hawaii is accredited by the Accrediting Commission for Senior Colleges and Universities of the Western Association of Schools and College.
Sunday, October 31, 2010
Top Medical Schools in Netherlands
List of top medical schools in Netherlands:
University of Groningen
- The faculty of Medical Sciences of the University of Groningen is the second oldest medical faculty in The Netherlands.
- Graduates of the Bachelor’s programme in Medicine, Global Health profile can continue with the Master of Medicine programme (in Dutch) of the University of Groningen. Completion of this Master’s programme
University of Groningen
- The faculty of Medical Sciences of the University of Groningen is the second oldest medical faculty in The Netherlands.
- Graduates of the Bachelor’s programme in Medicine, Global Health profile can continue with the Master of Medicine programme (in Dutch) of the University of Groningen. Completion of this Master’s programme
Saturday, October 30, 2010
List of Medical Schools in Philippines
University of Santo Tomas Faculty of Medicine and Surgery is the first medical school in the Philippines. It is highly regarded as one of the top performing medical schools in the Philippines. The Santo Tomas Journal of Medicine is accredited by the Institute for Scientific Information and listed in the Index Medicus.
The University of the Philippines Manila is a Commission on Higher Education (
The University of the Philippines Manila is a Commission on Higher Education (
Online Schools of Nursing - Getting A Nursing Degree
Earning a nursing degree from online schools of nursing is becoming more and more popular. The flexibility and versatility these online nursing schools offer poses a lot of benefits.
Those looking to get a nursing degree can definitely take advantage of all the benefits online schools of nursing have to offer.
When earning a nursing degree online, you basically complete the non-clinical courses because clinical and laboratory classes
must be completed in person at a medical facility also operated by the online school of nursing. It is important to know that there are no online nursing programs that allow you to fully complete the degree online. Nevertheless, it is one good way to become a registered or practical nurse.
To find online nursing schools such as online practical nursing schools, you need to do a little research online. There are many websites offering online nursing courses. In fact, even online nursing PHD programs are available on the Internet. On Google or even on other reliable search engines, type the keywords that will help you find the online nursing schools you would like to attend. At the very least, you can type the words "online nursing degree" or "nursing degree online". You may also type the name of your city or state that you would like your nursing program to be in. The search engine will show you results with links to many online nursing schools. Check out some of these sites to see in detail what they offer and find out if their offerings match what you are looking for. There are some things that you consider when choosing the online school to attend to.
First and foremost, find out if the nursing program allows you to work at your own pace or the one that follows the school's schedule. A program that allows you to work at your own pace will allow you to finish or complete the work at a schedule or pace that suits you. However, there are many nursing programs structured like a traditional school or college. You should also find out the date when you can start. Some online schools for nursing have rolling enrollment which means that you can start at any date you prefer. Others designate a starting date.
You should also check if the online school has an academic advisor. It is a good idea to settle for one that assigns an academic advisor for each student because the advisor will help and work with students closely to help in planning out the course of study. An academic advisor also helps students keep on tract, connects with the students online, and coordinates with the students' clinical classes.
You should also check the costs of the nursing program because not all schools have the same charges. A thorough search of programs will help you land on the most affordable yet right online school for you. It is also good if you can find out if the school offers financial assistance. Many online nursing programs offer assistance and it is a good idea to take advantage of this financial help.
Once you have completed your research
 , you can narrow your choices of online schools of nursing down to a few until you land on the best one.
, you can narrow your choices of online schools of nursing down to a few until you land on the best one.
Nurse Practitioner Jobs OG/GYN jobs NP jobs
NP jobs PA jobs Nurse Practitioner Jobs, Physician
Assistant jobs, Advanced Practice Jobs, ARNP jobs, Nurse Practitioner
Resumes, Nurse Jobs, Physician Jobs, CRNA jobs, Advanced Registered
Nurse Practitioner Jobs,Advanced Practice Provider,Advanced Practice
Clinician,
Top MBA in Czech Republic
List of top MBA schools in Czech Republic:
Prague International Business School
- It offers three forms of study for the degree of Master of Business Administration (MBA): Residential form; In-Business form; Distance form of study.
- The residential MBA study is organized in such a way that it makes maximum use of interpesonal communication to achieve synergic effect resulting from team work of
Prague International Business School
- It offers three forms of study for the degree of Master of Business Administration (MBA): Residential form; In-Business form; Distance form of study.
- The residential MBA study is organized in such a way that it makes maximum use of interpesonal communication to achieve synergic effect resulting from team work of
Yes We Can
SUCH is Scottish popular culture that if either STV or BBC Scotland were ever to raise the comedy bar beyond "couthy" and come up with something akin to the legendary 'Four Yorkshiremen' sketch (Four Fifers anyone?), there would have to be a football element.
I could see the Pars' fan putting-up Alex Edwards, Alex Ferguson, Willie Cunningham and Jackie Sinclair; back would come the East Fifer weighing-in with Allan Brown, "Legs" Fleming, George Aitken and Jimmy Bonthrone; only to be trumped by the two-word response from the Starks Parker: "Jim Baxter".
I slalom down this back road of whimsey after looking at a piece in this morning's Scotsman, in their 'From the Archives' feature. This is a great wallow in nostalgia, I just wish Donald Walker and his terrific team on the Hootsman's sports desk would up their production values and try to find archive features matching the date of use.
As an Ayrshireman I'm always happy to read about triumphs by Ayrshire sides and today's was all about that glorious day, 24 April, 1965, when Killie went to Tynecastle, won 2-0 and lifted the League Championship for the only time.
Worth celebrating certainly, but maybe not specifically in October, 2010. But, enough carping, that great win got me thinking. Back in 1965, that victorious Kilmarnock team contained just one current Scotland cap (i.e. one player who had played for Scotland that season) - centre half Jackie McGrory. Yes, injured goalkeeper Campbell Forsyth was also capped that season, while Bobby Ferguson, the young reserve whose late save from Alan Gordon secured the title would go on to be capped the following season. Right back Andy King was an Under-23 regular, Tommy McLean would go on to greatness, but for the rest, Under-23 or Scottish League recognition would be the best they could hope for; while such as Matt Watson were scandalously overlooked for any representative honours.
The Hearts team they beat also included one just one current Scotland cap, Willie Wallace, who had made his debut against Northern Ireland earlier that season; but the Hearts XI also included an already capped goalkeeper in Jim Cruickshanks, Davie Holt, capped at left back the previous season and various players such as Billy Higgins, Roy Barry and Johnny Hamilton who had played in Under-23 or League internationals.
Dunfermline finished third with a squad similarly lacking in international names: then came Hibs, whose only capped player that season, Neil Martin, didn't make his Scotland debut until the following month. Rangers, who then as now could have fielded a team of full internationalists were fifth, while Celtic, managed by Jock Stein and with all bar Wallace and Ronnie Simpson of the Lisbon Lions already in place and five current Scotland internationalists in their ranks finished that season eighth, behind Dundee and Clyde.
Back then, the provincial clubs already were at a fiscal disadvantage against the Old Firm - they were always at the mercy of English raiders, picking-off their better players, but, they competed, they gave the Big Two a run for their money and beat them more often than they do today.
I would suggest that notwithstanding their huge advantage in support, it ought to be easier to compete with the Old Firm today. Back then, Celtic and Rangers could afford to pay more than most English First Division sides; then as now, they could offer virtually-guaranteed European football - they would not have lost first team players to Second Division sides in England (Championship sides today). The playing field is flatter today, every Scottish club is vulnerable to player loss because of the riches in the south.
But, in spite of this, the Old Firm is more dominant than ever.
WHY?
Where is the determination from club directors and managers to get their players to have a real go at the big two? There are riches to be had for the first club brave enough and determined enough to say: "We can beat them".
I long to see another 1965, with the Old Firm trotting in with the other also-rans, what a boost that would be for Scottish football.
Where is Scottish football's Obama? - crying out: "Yes We Can".
Latest hairstyles, can support your performance to appear more confident

Various latest hairstyles began to dare to be combined and introduced, among which:
1. Le Graphic, inspired by a harmonious alignment, from light to dark, soft to hard, extreme elegance and imagination crazy, Carney and Pemberton combines classic cutting and coloring as well as the principles of artistic ingenuity to create strength, linear framework for vivid colors .
2. Le Cuts, is a merger of the main concepts in a J-Cutting ketidakterdugaan and sometimes cut off, creating an elegant hair style, bold and timeless.
3. Le Colors, inspired by the innovative use of color and graphical form. Artistic Director Vero K-PAK incorporates various levels and intensity of it to put them in place of the base construction.
The colors produced shades of gold, copper, cool red, and purple, with a blend of contrasting color at the same time it produces a smooth color and graphics.
While the colors of shades of blonde hair styles, lavender, and blue to produce color with greater clarity and color techniques expose glacial interpretation.
It's time you switch with the latest hairstyles.
Happy Blogging!
Friday, October 29, 2010
Top MBA Programs in Bangladesh
List of top MBA program providers in Bangladesh:
Asian University of Bangladesh (AUB)
- It has the largest School of Business among the private universities in Bangladesh.
- The Master of Business Administration (MBA) program has been designed to enroll students of various backgrounds.
- The Internship is a part of the MBA degree requirement for fresh students who do not have work experience.
Asian University of Bangladesh (AUB)
- It has the largest School of Business among the private universities in Bangladesh.
- The Master of Business Administration (MBA) program has been designed to enroll students of various backgrounds.
- The Internship is a part of the MBA degree requirement for fresh students who do not have work experience.

PHYSICAL Therapists/OCCUPATIONAL Therapists PTA'sCOTA Speech Therapist (SF Bay Area)
ON-CALL THERAPISTS is a REGISTRY in the San Francisco Bay Area since 1981.
IMMEDIATE JOB OPPORTUNITIES!
WE HIRE: PHYSICAL THERAPISTS (RPT)
OCCUPATIONAL THERAPISTS (OTR)
SPEECH THERAPISTS (SP)
PHYSICAL THERAPISTS ASSISTANTS (PTA)
OCCUPATIONAL THERAPISTS ASSISTANTS (COTA)
FULL time or PART TIME WORK available IMMEDIATELY! We have EXCELLENT benefits for full time employees. Medical and Dental. 401K plan.
LICENSED IN THE STATE OF CALIFORNIA!
Work Settings are in: ACUTE CARE, ACUTE REHAB, SKILL NURSING, OUT PATIENT FACILITIES, HOME HEALTH!
Work when you want to work. Small Company with a personal touch. Come join our team!
Call Lynn at (510)569-9884 Fax (510)569-9886.
WEB SITE: on-calltherapists.com
(IMMEDIATE JOB OPPORTUNITIES)
Email. mailto:oncallther@aol.com?subject=PHYSICAL Therapists/OCCUPATIONAL Therapists PTA'sCOTA Speech Therapist (SF Bay Area)&body=http://sfbay.craigslist.org/eby/hea/2031660601.html
IMMEDIATE JOB OPPORTUNITIES!
WE HIRE: PHYSICAL THERAPISTS (RPT)
OCCUPATIONAL THERAPISTS (OTR)
SPEECH THERAPISTS (SP)
PHYSICAL THERAPISTS ASSISTANTS (PTA)
OCCUPATIONAL THERAPISTS ASSISTANTS (COTA)
FULL time or PART TIME WORK available IMMEDIATELY! We have EXCELLENT benefits for full time employees. Medical and Dental. 401K plan.
LICENSED IN THE STATE OF CALIFORNIA!
Work Settings are in: ACUTE CARE, ACUTE REHAB, SKILL NURSING, OUT PATIENT FACILITIES, HOME HEALTH!
Work when you want to work. Small Company with a personal touch. Come join our team!
Call Lynn at (510)569-9884 Fax (510)569-9886.
WEB SITE: on-calltherapists.com
(IMMEDIATE JOB OPPORTUNITIES)
Email. mailto:oncallther@aol.com?subject=PHYSICAL Therapists/OCCUPATIONAL Therapists PTA'sCOTA Speech Therapist (SF Bay Area)&body=http://sfbay.craigslist.org/eby/hea/2031660601.html
Dense Doctors

That title may sound a bit harsh. I know that our doctors are very intelligent when it comes to medicine.
But apart from that they seem to know sweet fuck all.
This is especially true when it comes to what is going on in the wards. It is true in regards to Nursing. If Nursing care goes bad medical orders do not get carried out and patients do not get monitored. In short the doctor's whole plan of care goes out the fucking window.
You would think that they would be a little more......well.....interested.
But no. They are delusional.
This is what I have learned about doctors in over a decade of Nursing.
1. They think all nurses are the same person or clones of the same person with a hive mind.
For example, if the Nurse on the shift before you missed something, it's your ass if you are the one on duty when doc graces your ward with his presence. If you are forced to float to a specialty you never worked or trained in before the doctors expect you to telepathically mind link with absent Nurses who have experience that area the minute you arrive on the ward They will not bother to write their orders or give you a heads up about things you need to know and wouldn't know unless you have experience there. They won't bother with any of that yet they'll go apeshit later when you forgot to remind them to prescribe something. Remember that they think Nurses are all the same drone with a hive mind who know each Doctors' individual ways.
2. They have no idea how to implement their own orders, or how time consuming and complex it is to implement their own orders.
Don't even get me started on the bullshit with the IV meds....both getting a hold of them and actually preparing them. Or fighting with pharmacy, equipment library and path lab. No Doctor they do not just keep everything on the ward for us. No they do not keep chest tube kits in a place where we can get them etc etc etc.
3. They have no idea how to work the system as a result of the Nurses doing it for them.
They don't understand why things don't happen instantly. For example, all RN's know it takes 6 weeks to get a patient into a Nursing home and that nothing can be done to speed this process up. Yet day after day the medical consultant walks in the very afternoon after he wrote that 90 year old Mabel can be discharged that morning and wants to know why she is still on the ward. Then he goes on a rant about how the Nurses can't be arsed to discharge patients. I could go on and on about this one, there are thousands of examples.
4. The saddest thing I learned about doctors and the crux of this post is that doctors are not able to distinguish between Nurses and ward assistants.
There are many times I am running my ass off trying to give a 150 IV meds all due now whilst the HCA's/cadets/auxiliaries are hanging out at the Nurse's station. The few jobs they can do are complete. They cannot help with the large proportion of the workload that only an RN can handle. Many doctors will walk onto a ward, take a look at the assistants hanging out at the station and exclaim "The Nurses don't seem to busy today". Dickhead. I am the only Nurse, and I am on my knees completely overwhelmed. What the assistants are doing (or not doing) is in no way indicative of how busy the Nurses are! Assistants are not Nurses.
Sometimes I will be 3 hours behind getting much needed drugs into patients and managing other patient problems and some young doctor will stroll onto the ward and ask me to hold an arm for him so that he can draw some ABGs. For god's sake, grab one of the assistants hanging around the Nurse's station for that. That is something they can actually do. Don't delay Mrs. Smith's pain relief any longer by causing me to stop and hold an arm!! It's not like the care assistants can give the meds and handle the Nurse stuff while I am tied up holding an arm for you!
A doctor walked onto my ward and wrote some orders for IV fluids and IV antibiotics for a patient with Pneumonia. As the only Nurse for all of those patients I was tied up and didn't see him arrive or know he wrote any orders. He handed the chart with his orders to a care assistant and left the ward. The care assistant has no idea about orders etc. She put the chart down on the station where it got immediately buried. And she said nothing to me. I had 25 patients that day (a staffing ratio no Nurse can function well with) and it was taking a hell of a lot of time to see everyone and process their orders. It was 3 hours before (by luck) I found the chart and the orders. Patient was in septic shock by that point. Doctors, you need to tell the actual Nurse about these things, not some underpaid teenage assistant that you have confused with Nursing staff.
Then there was the doctor who started yelling at me for having 4 bays full of patients rather than one!! "That is too many patients! You should have one bay per Registered Nurse". Yes Sherlock, no shit. I appreciate the fact that you have actually noticed that the RN ratios on NHS wards are horrible and dangerous and that this has a dire effect on patient care. But what the hell would possess you to think that they Nurses on the ground have any say in how we are staffed or how many patients we have? Even the ward Sisters are not allowed to have a say in how their wards are staffed. Duh.
I could go on and on. These doctors are clueless about what is going on with Nursing care and RN staffing on the wards. And frankly, I am getting sick of it.
My cousin in law is a doctor in the USA. He is not as dense as his colleagues here. If he finds out that his patients' RN's are being forced to take on more than 4-6 patients at a time he gets on the phone to MANAGEMENT and starts screaming. He tells management that he will have his patients pulled out of there by the end of the day and admitted somewhere else if they do not staff the facility properly.
He doesn't care how compassionate or knowledgeable or wonderful the Nurses are in that place. He knows that with poor staffing ratios that they cannot function even if they are wonderful. The facility would lose a ton of money if he pulled his patients out of there so they wouldn't dare short staff the place. They did it once, never again. Managers of hospitals all over the world think that intentional RN short staffing is the way to save cash.
He is a good doctor, and understands that without decent Nursing care delivered by RN's the patients are screwed. He understands that there will be nothing in the way of decent Nursing care in a place where Nurses are denied resources and safe staffing ratios. And he acts on it.
But it seems it is too much to ask for UK doctors to even understand what a Nurse is, let alone stand up for them. They haven't even grasped the notion that these Nurses are taking on too many patients to be able to care for anyone properly, and that they are being forced into a position where they cannot spend two minutes demonstrating compassion without risking a disciplinary for not filling in paperwork. Too bad.
How To Get The Advanced Practical Nursing Job You Want (Ebook Killer Version)
How To Get The Advanced Practical Nursing Job You Want (Ebook Killer Version)
“How To Get A Job You Want And Succeed Once You’re There,” has been
edited only for those interested this particular job. This ebook contains helpful
tips for keeping a job, interviewing, a resume template all ready to go, and
very comprehensive information regarding the career field from job growth, to
educational requirements, to the very nature of the job, and everything in
between. Get the job you want with the information in this ebook!
THIS EBOOK HAS BEEN FORMATTED INTO A SIMPLIFIED VERSION SO IT
IS NOW COMPATIBLE WITH SMARTPHONES. GRAPHICS HAVE BEEN
OMITTED FOR A SIMPLIFIED TEXT READING EXPERIENCE.
(EBOOK KILLER VERSION INFORMATION) Ever notice that most ebooks
have basically the same information? Hell, even sometimes they have the
same information word-for-word? That's because all of those ebooks use the
same couple of sources for their information, and all they do is re-write a
couple or articles or chapers, and then click "publish." With an "Ebook Killer
Version," we're giving you all of the original, unedited information used to
create those ebooks so you don't have to keep buying the same stuff over and
over again. We're going to give you everything, even if some of the chapters
seem like duplicates, so you can save your money.
Click Here 

Product Description
Do you know what it takes to get the job you want? In this ebook, the original“How To Get A Job You Want And Succeed Once You’re There,” has been
edited only for those interested this particular job. This ebook contains helpful
tips for keeping a job, interviewing, a resume template all ready to go, and
very comprehensive information regarding the career field from job growth, to
educational requirements, to the very nature of the job, and everything in
between. Get the job you want with the information in this ebook!
THIS EBOOK HAS BEEN FORMATTED INTO A SIMPLIFIED VERSION SO IT
IS NOW COMPATIBLE WITH SMARTPHONES. GRAPHICS HAVE BEEN
OMITTED FOR A SIMPLIFIED TEXT READING EXPERIENCE.
(EBOOK KILLER VERSION INFORMATION) Ever notice that most ebooks
have basically the same information? Hell, even sometimes they have the
same information word-for-word? That's because all of those ebooks use the
same couple of sources for their information, and all they do is re-write a
couple or articles or chapers, and then click "publish." With an "Ebook Killer
Version," we're giving you all of the original, unedited information used to
create those ebooks so you don't have to keep buying the same stuff over and
over again. We're going to give you everything, even if some of the chapters
seem like duplicates, so you can save your money.
Click Here
Maternal Child Nursing Care - Text and E-Book Package
Maternal Child Nursing Care - Text and E-Book Package

The Evolve eBook gives you electronic access to all textbook content with plenty of added functionality. Not only can you search your entire library of eBooks with a single keyword, you can create your own customized study tool by highlighting key passages, taking and sharing notes, and organizing study materials into folders. Add additional eBooks to your collection to create an integrated digital library! Your Evolve eBooks are conveniently accessible either from your hard drive or online.
Book Description
This market-leading textbook provides just the "right amount" of maternity and pediatric content in an easy-to-understand manner. Divided into two sections, the first part of the book includes 28 chapters on maternity nursing and the second part contains 27 chapters covering pediatric nursing. Numerous illustrations, photos, boxes, and tables clarify key content and help you quickly find essential information. And because it's written by market-leading experts in maternity and pediatric nursing, you can be sure you're getting the accurate, practical information you need to succeed in the classroom, the clinical setting, and on the NCLEX® examination.
Maternal Child Nursing Care - Text and E-Book Package

Product Description
Evolve eBookThe Evolve eBook gives you electronic access to all textbook content with plenty of added functionality. Not only can you search your entire library of eBooks with a single keyword, you can create your own customized study tool by highlighting key passages, taking and sharing notes, and organizing study materials into folders. Add additional eBooks to your collection to create an integrated digital library! Your Evolve eBooks are conveniently accessible either from your hard drive or online.
Book Description
This market-leading textbook provides just the "right amount" of maternity and pediatric content in an easy-to-understand manner. Divided into two sections, the first part of the book includes 28 chapters on maternity nursing and the second part contains 27 chapters covering pediatric nursing. Numerous illustrations, photos, boxes, and tables clarify key content and help you quickly find essential information. And because it's written by market-leading experts in maternity and pediatric nursing, you can be sure you're getting the accurate, practical information you need to succeed in the classroom, the clinical setting, and on the NCLEX® examination.
Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care
Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care

Book Description
Write individualized care plans with ease and confidence!
Product Description
Use this convenient resource to formulate nursing diagnoses and create individualized care plans! Updated with the most recent NANDA-I approved nursing diagnoses, Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 9th Edition shows you how to build customized care plans using a three-step process: assess, diagnose, and plan care. It includes suggested nursing diagnoses for over 1,300 client symptoms, medical and psychiatric diagnoses, diagnostik procedures, surgical interventions, and clinical states. Authors Elizabeth Ackley and Gail Ladwig use Nursing Outcomes Classification (NOC) and Nursing Interventions Classification (NIC) information to guide you in creating care plans that include desired outcomes, interventions, patient teaching, and evidence-based rationales.- Promotes evidence-based interventions and rationales by including recent or classic research that supports the use of each intervention.
- Unique! Provides care plans for every NANDA-I approved nursing diagnosis.
- Includes step-by-step instructions on how to use the Guide to Nursing Diagnoses and Guide to Planning Care sections to create a unique, individualized plan of care.
- Includes pediatric, geriatric, multicultural, and home care interventions as necessary for plans of care.
- Includes examples of and suggested NIC interventions and NOC outcomes in each care plan.
- Allows quick access to specific symptoms and nursing diagnoses with alphabetical thumb tabs.
- Unique! Includes a Care Plan Constructor on the companion Evolve website for hands-on practice in creating customized plans of care.
- Includes the new 2009-2011 NANDA-I approved nursing diagnoses including 21 new and 8 revised diagnoses.
- Illustrates the Problem-Etiology-Symptom format with an easy-to-follow, colored-coded box to help you in formulating diagnostic statements.
- Explains the difference between the three types of nursing diagnoses.
- Expands information explaining the difference between actual and potential problems in performing an assessment.
- Adds detailed information on the multidisciplinary and collaborative aspect of nursing and how it affects care planning.
- Shows how care planning is used in everyday nursing practice to provide effective nursing care.
Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care
NP jobs Nurse Practitioner Jobs PA jobs
NP jobs PA jobs Nurse Practitioner Jobs, Physician
Assistant jobs, Advanced Practice Jobs, ARNP jobs, Nurse Practitioner
Resumes, Nurse Jobs, Physician Jobs, CRNA jobs, Advanced Registered
Nurse Practitioner Jobs,Advanced Practice Provider,Advanced Practice
Clinician,
Top Medical Schools in South Africa
Following are the top leading medical schools in South Africa:
University of Cape Town Faculty of Health Sciences
- The Faculty of Health Sciences at UCT has the oldest medical school in Southern Africa. It offers undergraduate and postgraduate courses/programs over a wide range of healthcare-related disciplines.
- The Department of Medicine of the University of Cape Town is a large academic and
University of Cape Town Faculty of Health Sciences
- The Faculty of Health Sciences at UCT has the oldest medical school in Southern Africa. It offers undergraduate and postgraduate courses/programs over a wide range of healthcare-related disciplines.
- The Department of Medicine of the University of Cape Town is a large academic and
Nursing Care Plan | NCP West Nile Virus Infection
West Nile virus (WNV) infection is a disease spread by mosquitoes. Severe forms of the infection may be called West Nile encephalitis (if brain tissue is inflamed) or West Nile meningitis (if the membranes covering the brain become inflamed).
West Nile virus infection is caused by a virus related to those that cause yellow fever and dengue. It can be classified as a zoonosis because it is a disease that can be spread to humans from animals. It is also called an emerging infectious disease (EID) because it has become more widespread in the last 20 years and is likely to become more common in the future. Most people who become infected with the virus have no noticeable symptoms; about 20 percent develop a mild flu-like illness that lasts about a week; a few people develop a serious illness as a result of WNV causing inflammation of the central nervous system (the brain and spinal cord).
West Nile virus is increasingly widespread in both tropical and temperate regions of the globe. In North America, epidemics of WNV are most likely to occur in August and September, when mosquitoes are most active. The disease is not a serious infection in 80 percent of people exposed to it; out of 151 people who become infected with the virus, 110 will not notice any symptoms at all; forty will be sick for about a week; and one person will become severely ill. The risk of severe illness in North America is greatest among people over fifty, pregnant women, people who have recently had cancer chemotherapy, people with diabetes, and people with weakened immune systems. As far as is known, West Nile virus affects all races and both sexes equally.
The West Nile virus is thought to have developed in Uganda about a thousand years ago. It was first identified as a distinct cause of disease in 1937 in a feverish woman in central Africa by researchers who were studying yellow fever. WNV was not described as a cause of severe disease in older adults until an outbreak took place in Israel in 1957. The virus reached North America some time in the 1990s; the first outbreak that attracted public attention occurred in New York, New Jersey, and Connecticut in 1999. The disease has since been reported across the United States. According to the Centers for Disease Control and Prevention (CDC), the total number of deaths in the United States from WNV between 1999 and 2007 is 1,060; most have been in elderly people.
Nursing Care Plan Signs and Symptoms
West Nile virus infection is caused by a virus transmitted from infected birds to humans through mosquitoes that first bite the birds and then bite people. Crows, ravens, robins, and blue jays are the birds most likely to carry the virus; the CDC reported in 2007 that at least 138 different species of birds in North America have been found to carry West Nile virus, and forty-three different species of mosquitoes. The first major outbreak of West Nile infection in the United States was preceded by the sudden death of large numbers of birds in the New York City area.
The virus can be transmitted by mosquitoes to bats, horses, dogs, cats, squirrels, skunks, and rabbits as well as to people. The mosquitoes that carry the virus are called vectors, and the infected animals that harbor the virus are called hosts. The virus can also be transmitted by blood transfusions, organ transplants, and from a nursing mother to her baby through breast milk. People cannot get West Nile virus, however, by touching or kissing someone with the virus; there are also no reported cases of people getting West Nile infections from household pets. When a mosquito carrying WNV bites a human, the virus is transmitted directly into the bloodstream. Once in the bloodstream, WNV multiplies for an incubation period of three to fourteen days. The 20 percent of people who feel symptoms of WNV infection typically have chills, a low-grade fever, headache, sore throat, and nausea and vomiting. About half these patients will also develop a mild rash on the upper chest. In most cases the illness lasts about a week, although the person may feel tired for several weeks afterward.
West Nile encephalitis or meningitis develops when the virus reaches the tissues of the brain or the tissues that cover the brain and the spinal cord and multiplies there. People with this severe form ofWest Nile infection develop a stiff neck, severe headaches, and feel mentally confused. They have weak or partially paralyzed muscles and may lose consciousness.
Nursing Care Plan Diagnosis
The symptoms of West Nile virus are similar to those of other viral infections. A definite diagnosis can be provided by testing blood or spinal fluid for antibodies against the virus. Since 2003, the Food and Drug Administration (FDA) has approved two rapid diagnostic tests for detecting the West Nile virus; one, developed in Australia, gives results in two hours. The other test was developed in Canada and was approved for use in the summer of 2007; it gives results in only fifteen minutes.
Nursing Care Plan Treatment
There is no specific treatment for West Nile virus. Most people who develop fever, nausea, or other symptoms recover without seeing a doctor because the symptoms are similar to those of other mild viral infections. The National Institute of Allergy and Infectious Diseases (NIAID) is
currently testing a new drug treatment for WNV that was expected to complete its Phase I clinical trial by the end of 2008.
People who develop West Nile encephalitis or West Nile meningitis should be taken to the hospital for specialized treatment to help them breathe. They may also be given intravenous fluids to prevent dehydration and intensive nursing care.
Prognosis
Most people who have a mild form of West Nile virus infection recover in about a week with no long-term health problems. Those with severe infections, however, have a 10 percent risk of dying. Those who survive may suffer permanent brain damage or paralysis similar to that caused by polio.
Nursing Care Plan Prevention
There is no vaccine against WNV for humans that has completed clinical trials, although a vaccine for horses has been developed and approved for use. The most important precautions that humans can take are controlling mosquitoes and preventing themselves from being bitten by mosquitoes.
The CDC recommends the following steps:
• Once a week, drain water from birdbaths, outdoor buckets, flower pots, swimming pool covers, and other water-filled containers where mosquitoes can lay their eggs and breed. Empty children’s wading pools when they are not being used.
• Use insect repellent when outdoors; apply it to exposed skin and spray clothing with repellent.
• Wear long-sleeved shirts and long pants when the weather permits.
• Try to stay indoors in early morning and early evening, because mosquitoes are most active at those times of day.
• Keep window and door screens in good repair so that mosquitoes cannot get inside the house.
• Cover baby strollers or carriers with mosquito netting when taking the baby for a walk outdoors.
• Do not handle any dead birds found outside. Contact the local health department first and ask for instructions on reporting and disposing of them.
The Future
It is likely that a vaccine for humans and a specific treatment for West Nile virus will be approved by the FDA within the next few years. About 450 different chemicals that appear to be effective against viruses have been identified since 2003 as promising enough to justify further testing. There were also two potential vaccines against WNV undergoing clinical trials at the NIAID Vaccine Research Center in Maryland in 2008.

Thursday, October 28, 2010
San Francisco, Bodega Bay, Petaluma, Santa Rosa
Just got back from a self-assigned vacation. My BFF got married... and I ditched 10 days of the GI block... opting for a hiatus instead. Wine tasting, pampering, champagne, bachelorette parties, etc. Here's a few shots.




Not So Much Cool as a Cuke
Last night I was a patient. And a freaked out one. So this is probs TMI, but it's my blog and I don't care. So I occasionally get a UTI. Maybe once every few years. But they are always solved within an hour by drinking a couple of big glasses of water. No biggie. But last night it didn't work. It just got worse. And worse. And eventually I started peeing blood. And then I panicked. Like panicked panicked. WTF? I knew I wasn't going to die. Well I kinda felt like it, but I knew logically I wouldn't. And the other thing. I had this horrible realization that I was alone. Like really alone. Who should I call at 2:00am? Lolo had to work in the morning... and what could she do? Dr J was sleeping... and though I called him he didn't pick up. I was seriously in too much pain to go to the ER or urgent care. And Mr. Ex Boyfriend was on vacay with his new girlfriend. Not exactly great options.
An hour later it got worse and I sacked up and called my ex. He called me in an antibiotic and some azo. I'm sure his girlfriend was thrilled that he was doing me favs while on vacation. Oh well. Then I woke up my neighbor to run to Walgreens for me. Which he nicely did. That was pretty major for me actually. I have some crazy psychosis where I am practically physically incapable of asking other people for favors. But I did. And they said yes. So thank you Eli and my neighbor. You saved my ass.
Orgasmic Hospital Birth? Tell us about it!
Have you had an ecstatic and/or orgasmic hospital or clinic birth experience?
We would love to hear about it- and print it! Spread the word!
The submission deadline for the winter issue is Nov 15th 2010!
submissionstosquat@gmail.com
Love
SQUAT
We would love to hear about it- and print it! Spread the word!
The submission deadline for the winter issue is Nov 15th 2010!
submissionstosquat@gmail.com
Love
SQUAT
University of Cape Town - Rankings
Founded in 1829, the University of Cape Town (UCT) is a top ranking public university located in Cape Town in the Western Cape province of South Africa. It is the oldest university in South Africa.
UCT has become a partner in the Worldwide Universities Network (WUN), making it the first African member of this global network. WUN is a partnership of research-led universities from North America,
UCT has become a partner in the Worldwide Universities Network (WUN), making it the first African member of this global network. WUN is a partnership of research-led universities from North America,
The Mental Status Exam
The mental status exam, is an assessment tool that helps identify psychological symptoms that may assist the practitioner determine if there is a psychogenic problem. When assessing mental status, it is important to adjust questions and categories to avoid age and/or cultural bias.
Category Description Appearance General appearance, grooming and gait. This is best observed as the client comes into the room. Grooming is one of the earliest areas to deteriorate when mental function has diminished. Behavior Speech, eye contact, body language, response to the environment. Observe for appropriate use of personal space. Does the person come right into your face, or stand an unusual distance away. Insight The ability of the client to be aware of one’s own abilities. The ability to analyze a problem objectively. Ask the client to explain a problem. Intellectual Functioning Simple calculations, ability to abstract or think symbolically and categories of association. This is done through direct questioning using math, proverbs or analogy. Judgment Assesses decision-making abilities. Ask client What he would do in a dilemma regarding an important decision. Memory Immediate recall, recent memory, remote memory. Ask the client about a recent current event that both you and the client should know. Ask about some event in the past that should be known by both. Be very careful in this area to avoid cultural bias. Mood and Affect Mood relates to the emotions of the moment while affects refers to the range of emotions displayed such as happy, sad, or unchanging. Compare in relation the client’s probable everyday behavior. Orientation Assess for awareness of person, time, place, and purpose. Perceptual Processes Awareness of self and one’s thoughts, reality and fantasy. Ask about delusions, illusions and hallucinations. Do not hesitate do ask direct questions. Sensorium Ability to concentrate, perception of stimuli. Thought Contents This assesses themes in conversation and is assessed by observing what the client discusses spontaneously in conversation. Thought Processes This measures a stream of conscious or mental activity as indicated in speech. Observe for rate, flow, and ability to pursue a topic logically.
www.accessce.com
Neurological Assessment : Checks Pupils
Neurological Assessment : Checks Pupils

- Observes Both Pupils Simultaneously For: Equality, Size and Shape.
- Compares pupils for equality.
- Determines size, dilated, constricted, pinpoint.
- Determines irregularities in shape.
- Observes Direct Pupillary Light Reflexes.
- Checks one pupil at a time.
- Shines flashlight into eye from side.
- Repeat other eye.
- Observes Consensual Pupillary Reflex
- Shines flashlight into each eye alternately.
- Observes opposite pupil. Opposite pupil should constrict when light shore.
- Charts description of pupils: Equality, size, shape, reaction to light.
- Observes pupillary response to accommodation
- Have patient follow a closer moving object such as a pen.
- Pupils will constrict (or accommodate) to the closer moving object. * cannot be tested on blind or confused persons.
- Observes Extraocular Movements
- Asks patient to focus on object.
- Moves object; medical, lateral, superior, inferior and circular. In the pattern of an "H."
- Observes movement of both eyes in each of above directions; notes abnormalities or weakness. A. Charts extraocular movements as "full" if no abnormalities or "unable to move eyes laterally, medially etc."
Do Flashy Campaigns Make a Difference for Breast Cancer?
by Melissa Garvey, ACNM Writer and EditorOctober is National Breast Cancer Awareness Month, and one Facebook campaign has already gone viral. It’s not a campaign imploring people to donate to breast cancer research. Instead, women are using their Facebook status updates to reveal where they like to put their purse.As you can imagine, this leads to all sorts of sexual connotations–for example, “I
Nursing Care Plan | NCP Vitiligo
Vitiligo is a skin disorder in which patches of skin—most commonly on parts of the body that are exposed to sunlight— lose their pigmentation. The patches of depigmented tissue may involve the soft tissues that line the nose and mouth.
Vitiligo is a skin disorder in which patches of skin, soft tissues lining the nose and mouth, and/or hair gradually lose their color. This loss of color takes place when melanin, a dark brown or reddish pigment produced by cells in the skin called melanocytes, is either destroyed or not produced in the first place. The patches of depigmented skin may grow, shrink, or stay the same size. They usually appear first on the parts of the body that are exposed to the sun, such as the hands, feet, face, lips, and arms. They may spread later to the armpits, genitals, groin area, and the soft tissues that line the nose and mouth. In some cases the white patches may eventually cover the patient’s entire body.
Doctors classify vitiligo into three types according to the pattern of the skin patches:
• Focal. The areas of depigmented skin are limited to one or a few parts of the body.
• Segmental. The loss of color occurs on only one part of the body.
• Generalized. There are many patches of white skin on many different parts of the body. This is the most common of the three patterns.
Vitiligo is thought to affect between 0.5 and 2 percent of people around the world, as many as 65 million adults. There are between 1 and 2 million people in the United States with the disorder. Vitiligo can start at any age, but roughly half of patients develop it before age twenty and most patients before age forty. It affects men and women equally, although women are more likely to notice the disorder at an earlier age than men. It also affects people of all races equally; however, the depigmented areas of skin are more noticeable on people with darker skin. In addition to humans, vitiligo is found in some animals, particularly certain breeds of dogs and horses.
Nursing Care Plan Signs and Symptoms
The causes of vitiligo are not completely understood. One reason some researchers think that genetic factors may be involved is that about 30 percent of cases run in families. Another theory is that vitiligo is either an autoimmune disorder or caused by one. Still other researchers think that vitiligo may be stress-related, because some people develop their first symptoms of it following a severe case of sunburn or an emotional shock. None of these theories have been proved so far, however.
In addition to the patches of depigmented skin, the symptoms of vitiligo may include:
• Premature graying (before age thirty) of scalp hair, pubic hair, and eyebrows.
• Uveitis. This is an inflammation of the interior of the eye.
• Depigmented areas on the soft tissues lining the mouth and nose.
• Change in color of the retina of the eye.
• Itching of the affected skin. This symptom is usually limited to the early stages of the disorder.
• Increased sensitivity to sun exposure.
Although vitiligo is a skin disorder and not a psychiatric condition, many patients do have
strong psychological reactions to the impact of the disorder on their appearance, particularly if the face is affected. In some cultures, people with vitiligo are thought to be evil or infected with leprosy and may be rejected by other members of the community. Many people with vitiligo in the United States become depressed or socially isolated because they are afraid of being stared at or teased.
Nursing Care Plan Diagnosis
The diagnosis of vitiligo is based on the patient’s history, including a family history of vitiligo. The doctor will also ask about autoimmune disorders, recent sunburns or other injuries to the skin, unusual sensitivity to the sun, or a history of diabetes.
In most cases the doctor can diagnose vitiligo by looking at the patient’s skin with a Wood lamp, a special device that uses ultraviolet light to diagnose skin infections and other abnormalities. Another diagnostic technique that can be used is the skin biopsy. To perform a biopsy, the doctor removes a small piece of the affected skin to examine under a microscope. If the patient has vitiligo, the skin sample will usually show a complete absence of melanocytes.
Nursing Care Plan Treatment
There is no cure for vitiligo. Medical or surgical treatment is not necessary; some people choose to manage the condition with special cosmetics that cover the white areas and even out the person’s skin tone. Even patients who choose medical or surgical therapies may wish to use camouflage cosmetics during their treatment, as it takes between six to eighteen months to complete treatment.
No treatment that is presently available for vitiligo will work for all patients. The choice of treatment depends partly on the number, size, and location of the white patches. Medical treatments for vitiligo are aimed at reducing the contrast between the pigmented and depigmented areas of skin. They include:
• Corticosteroids. These medications are applied directly to the depigmented skin; they work by restoring the color to the white areas. They take about three months for the skin to show improvement.
• PUVA (psoralen/ultraviolet A) therapy. In this type of treatment, the patient takes a drug called psoralen either by mouth or by applying it to the skin as a cream. The patient is then exposed to carefully timed ultraviolet light in the doctor’s office. Psoralen reacts with ultraviolet light to darken the skin. Major drawbacks of PUVA therapy are its side effects (chiefly sunburn and too much darkening of the skin) and an increased risk of skin cancer.
• Depigmentation. A drug called Benoquin is applied twice a day to the pigmented areas of the body to lighten them to match the areas that are already white. Depigmentation may be the best choice for people who have vitiligo onmore than 50 percent of the body. Its chief drawback is that the person’s skinwill always be unusually sensitive to sunlight afterward. In addition, this form of treatment is irreversible.
Surgical treatments for vitiligo include:
• Skin grafts. The surgeon removes skin from pigmented areas of the patient’s body and places it on depigmented areas. This procedure has a number of drawbacks: it is time-consuming, expensive, painful, and carries some risk of scarring and infection.
• Micropigmentation (tattooing). In this procedure, the doctor implants pigment into the skin with a special surgical instrument. It is usually used only in the area around the lips. One drawback is that it is usually difficult to match the patient’s natural skin color.
• Autologous melanocyte transplantation. This procedure is still considered experimental. The doctor removes a sample of the patient’s normal pigmented skin and places it in a special culture
medium to grow melanocytes. After the melanocytes have multiplied, the doctor transplants them into the areas of depigmented skin. As of 2008, this treatment was very expensive and impractical for most people with vitiligo. Patients with vitiligo are encouraged to join support groups or seek counseling in order to cope with the emotional effects of the disease.
Prognosis
It is very difficult to predict the spread of vitiligo on any patient’s body or
the outcome of any specific type of treatment.
Nursing Care Plan Prevention
There is no known way to prevent vitiligo, because the causes of the disorder are not yet understood.
The Future
It is not likely that vitiligo will become either more or less common in the general population than it is at present. Research into the disorder is focused on looking for specific genes that may be related to vitiligo and examining the role of stress in triggering the onset of the disorder. Some
evidence has been recently found of a link between vitiligo and variants of a gene called FOXD3.
Top Sociology Departments
Following are the top leading sociology departments in the UK:
The University of Essex
- It is the only Sociology department in the country to have been awarded the highest rating in all six of the national Research Assessment Exercises (RAE) that have been undertaken since 1986.
- In the RAE 2008, Essex Sociology achieved joint 1st position in the nation. 90% of our research was judged to be of
The University of Essex
- It is the only Sociology department in the country to have been awarded the highest rating in all six of the national Research Assessment Exercises (RAE) that have been undertaken since 1986.
- In the RAE 2008, Essex Sociology achieved joint 1st position in the nation. 90% of our research was judged to be of
Wednesday, October 27, 2010
Online Anthropology Degree Programs
Accredited universities offering Anthropology degree programs via online/distance learning:
University of North Texas
- UNT’s Department of Anthropology offers the online master’s program for those who are unable to attend an on-campus master's program due to geographic or work constraints. The program can be completed in three years. All courses are fully online.
- The department of
University of North Texas
- UNT’s Department of Anthropology offers the online master’s program for those who are unable to attend an on-campus master's program due to geographic or work constraints. The program can be completed in three years. All courses are fully online.
- The department of
Vital Signs - Blood Pressure
Blood Pressure

Blood Pressure : Pressure of blood against the walls of the arteries
Systolic : Number that is on the top, and when heart is contracting
Diastolic : Number that is on the bottom, and when heart is at rest
Systolic range : 90 - 140
Diastolic range : 60 - 90
Hypertension : High blood pressure, above 140 systolic or over 90 diastolic
Hypotension : Low blood pressure, under 90 over 60
To measure systolic : Sound of first beat
To measure diastolic : No beat is heard
Hypertension thickens heart muscle (hypertrophy) and reduces chamber in size
Thigh cuff for large arms, Small cuff pediatrics
Sphygmomanometer is instrument use to take blood pressure
Pulse pressure: Difference between systolic and diastolic
Vital Signs - Pulse
Pulse

Rate is : Number of beats per minute
Rhythm is : Regularity of beats
Normal range of adults : 60 - 100 per minute
Pulse : Can be weak, bounding or absent for short period of time
Rhythm : Can be regular or irregular
Palpate for : Rhythm, rate, and strength
Optimal finding : 80 per min. strong, and reg.
Tachycardia : Over 100 beats per minute
Bradycardia : Under 60 beats per minute
To measure pulse : count 30 sec.X 2
For irregular pulse : count the full 60seconds
Auscultate : Use stethoscope
Pulse deficit : Difference of apical and radial.
Vital Signs Respirations
Respirations

Respirations : How many breaths per minute
Adults: 12 - 20 / Infant slightly higher 20 - 40
Inhalation and Exhalation equals: 1 breath
To count breaths: Count 30 seconds by 2
Look for : Rhythm, rate, depth, and quality
Bradypnea: Under 12 breaths
Tachypnea: Over 20 breaths
Eupnea: Normal rate and depth
Apnea: Not breathing maybe 30 seconds or at all
Dyspnea: Difficulty in breathing
Orthopnea: Over bedside 90o postural position
Hyperpnea: Fast respirations
Cheyne Stokes: Increasing in rate and depth then periods of apnea - cyclic.
Kussmaul: Metabolic acidosis,usually the Diabetic. Rapid, very deep respirations intended to blow off carbondioxide.
Vital Signs - Temperature
Temperature
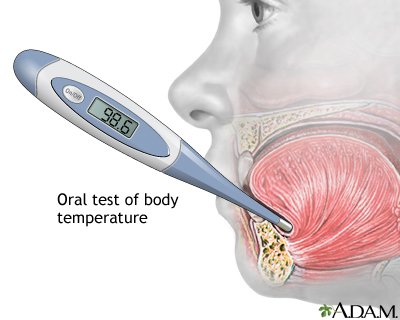
Oral - mouth
Time period 3 minutes
Normal range: 97.6 - 99.6 degrees
Absolute: 98.6 degrees
Rectal - Anus
Time period 3 minutes
Position -Lateral Sims
Normal range: 98.6 - 100.6 degrees
Absolute: 99.6 degrees
Axillary - Armpit
Time period 10 minutes
Normal range: 96.6 - 98.6
Absolute: 97.6 degrees
Otic or Tympanic Time period 10 sec. or less
Degree range is calibrated to rectal or oral
Hypothermia - Low body temperature
Hyperthermia - High body temperature
Pyrexia - High fever
Febrile - High fever
Afebrile - No fever
Things that can effect temperature: smoking, fluids, oxygen use, food, colds, or flu.(www.accessce.com)
Apgar Score
Apgar Scoring
| | | | | |
| | (Muscle tone) | | | |
| | (heart rate) | | | |
| | (response to smell or foot slap) | | | cry and withdrawal of foot (foot slap) |
| | (color) | | extremities blue | |
| | (breathing) | | weak crying | |
The total Apgar score is the sum of the scores for the five signs.
The 12 Cranial Nerves

There are 12 pairs of cranial nerves. These nerves arise from the brain and brain stem, carrying motor and or sensory information.
Cranial nerve I : Olfactory nerve
The olfactory nerve is composed of axons from the olfactory receptors in the nasal sensory epithelium. It carries olfactory information (sense of smell) to the olfactory bulb of the brain. This is a pure sensory nerve fiber.
Cranial nerve II: Optic nerve
The optic nerve is composed of axons of the ganglion cells in the eye. It carries visual information to the brain. This is a pure sensory nerve fiber. This nerve travels posteromedially from the eye, exiting the orbit at the optic canal in the lesser wing of the sphenoid bone. The optic nerves join each other in the middle cranial fossa to form the optic chiasm.
Cranial nerve III: Oculomotor nerve
The oculomotor nerve is composed of motor axons coming from the oculomotor nucleus and the edinger-westphal nucleus in the rostral midbrain located at the superior colliculus level. This is a pure motor nerve. It provides somatic motor innervation to four of the extrinsic eye muscles: the superior rectus, inferior rectus, medial rectus, and the inferior oblique muscles. It also innervates the muscles of the upper eyelid and the intrinsic eye muscles (the pupillary eye muscle.) Together, CN III, CN IV and CN VI control the six muscles of the eye.
Cranial nerve IV: Trochlear nerve
The trochlear nerve provides somatic motor innervation to the superior oblique eye muscle. This cranial nerve originates at the trochlear nucleus located in the tegmentum of the midbrain at the inferior colliculus level and exits the posterior side of the brainstem. It is also a pure motor nerve fiber.
Cranial nerve V: Trigeminal nerve
The trigeminal is the largest cranial nerve . It provides sensory information from the face, forehead, nasal cavity, tongue, gums and teeth (touch, and temperature) and provides somatic motor innervation to the muscles of mastication or “chewing”.
This cranial nerve has 3 branches: the ophthalmic, maxillary and mandibular branches.
It is composed of both sensory and motor axons. The sensory fibers are located in the trigeminal ganglion and the motor fibers project from nuclei in the pons.
Cranial nerve VI: Abducens nerve
The abducens nerve carries somatic motor innervation to one of the extrinsic eye muscles, the lateral rectus muscle. It is another pure motor nerve fiber and originates from the abducens nucleus located in the caudal pons at the facial colliculus level.
Cranial nerve VII: Facial nerve
The facial nerve carries somatic motor innervation to the many muscles for facial expression. It carries sensory information form the face (deep pressure sensation) and taste information from the anterior two thirds of the tongue. It arises at the pons in the brainstem and it emerges through openings in the temporal bone and stylomastoid foramen and has many branches. It is composed of both sensory and motor axons.
Cranial nerve VIII: Vestibulocochlear nerve
The vestibulocochlear nerve innervates the hair cell receptors of the inner ear. It carries vestibular information to the brain from the semicircular canals, utricle, and saccule providing the sense of balance. It also carries information from the cochlea providing the sense of hearing. This cranial nerve branches into the Vestibular branch (balance) and the cochlear branch (hearing). The cochlear fibers originate from the spiral ganglion. It is pure sensory nerve fiber.
Cranial nerve IX: Glossopharyngeal nerve
The glossopharyngeal nerve innervates the pharynx (upper part of the throat), the soft palate and the posterior one-third of the tongue. It carries sensory information (touch, temperature, and pressure) from the pharynx and soft palate. It carries taste sensation from the taste buds on the posterior one third of the tongue. It provides somatic motor innervation to the throat muscles involved in swallowing. It provides visceral motor innervation to the salivary glands. This cranial nerve also supplies the carotid sinus and reflex control to the heart . It is composed of both sensory and motor axons and originates from the nucleus ambiguous in the reticular formation of the medulla.
Cranial nerve X: Vagus nerve
The vagus nerve consists of many rootlets that come off of the brainstem just behind the glossopharyngeal nerve. The branchial motor component originates from the nucleus ambiguous in the reticular formation of the medulla. The visceral component originates from the dorsal motor nucleus of the vagus located in the floor of the fourth ventricle in the rostral medulla and in the central grey matt er of the caudal medulla. It is the longest cranial nerve
innervating many structures in the throat, including the muscles of the vocal cords, thorax and abdominal cavity. It provides sensory information (touch, temperature and pressure) from the external auditory meatus (ear canal) and a portion of the external ear. It carries taste sensation from taste buds in the pharynx. It also provides sensory information from the esophagus, respiratory tract, and abdominal viscera (stomach, intestines, liver, etc.). It provides visceral motor innervation to the heart, stomach, intestines, and gallbladder. It is part of the ANS, the parasympathetic branch. It is composed of both sensory and motor axons. Other parasympathetic ganglia include CN III , CN VII and CN IX .
Cranial nerve XI: Spinal Accessory nerve
The spinal accessory nerve has two branches. The cranial branch provides somatic motor innervation to some of the muscles in the throat involved in swallowing. This cranial branch is accessory to CN X, originating in the caudal nucleus ambiguous, with the fibers of the cranial root traveling the same extracranial path as the branchial motor component of the vagus nerve. The spinal branch provides somatic motor innervation to the trapezius muscles, providing muscle movement for the upper shoulders head and neck. It is pure motor nerve fiber.
Cranial nerve XII: Hypoglossal nerve
The hypoglossal nerve provides somatic motor innervation to the muscles of the tongue. This pure motor nerve originates from the hypoglossal nucleus located in the tegmentum of the medulla.
Source : www.pitt.edu
Normal Heart Sounds
Normal Heart Sounds

Heart Sounds
The heart sounds are the noises (sound) generated by the beating heart and the resultant flow of blood through it. This is also called a heartbeat. In cardiac auscultation, an examiner uses a stethoscope to listen for these sounds, which provide important information about the condition of the heart.
In healthy adults, there are two normal heart sounds often described as a lub and a dub (or dup), that occur in sequence with each heart beat. These are the first heart sound (S1) and second heart sound (S2), produced by the closing of the AV valves and semilunar valves respectively. In addition to these normal sounds, a variety of other sounds may be present including heart murmurs, adventitious sounds, and gallop rhythms S3 and S4.
Heart murmurs are generated by turbulent flow of blood, which may occur inside or outside the heart. Murmurs may be physiological (benign) or pathological (abnormal). Abnormal murmurs can be caused by stenosis restricting the opening of a heart valve, resulting in turbulence as blood flows through it. Abnormal murmurs may also occur with valvular insufficiency (or regurgitation), which allows backflow of blood when the incompetent valve closes with only partial effectiveness. Different murmurs are audible in different parts of the cardiac cycle, depending on the cause of the murmur.
Normal Heart Sounds
Normal heart sounds are associated with heart valves closing, causing changes in blood flow.
S1
The first heart tone, or S1, forms the "lubb" of "lubb-dub" or "lubb-dup" and is composed of components M1 and T1. Normally M1 precedes T1 slightly. It is caused by the sudden block of reverse blood flow due to closure of the atrioventricular valves, i.e. mitral and tricuspid, at the beginning of ventricular contraction, or systole. When the ventricles begin to contract, so do the papillary muscles in each ventricle. The papillary muscles are attached to the tricuspid and mitral valves via chordae tendineae, which bring the cusps or leaflets of the valve closed (chordae tendineae also prevent the valves from blowing into the atria as ventricular pressure rises due to contraction). The closing of the inlet valves prevents regurgitation of blood from the ventricles back into the atria. The S1 sound results from reverberation within the blood associated with the sudden block of flow reversal by the valves.[1] If T1 occurs more than slightly after M1, then the patient likely has a dysfunction of conduction of the right side of the heart such as a Right bundle branch block.
S2
The second heart tone, or S2, forms the "dub" of "lubb-dub" or "lubb- dup" and is composed of components A2 and P2. Normally A2 precedes P2 especially during inspiration when a split of S2 can be heard. It is caused by the sudden block of reversing blood flow due to closure of the aortic valve and pulmonary valve at the end of ventricular systole, i.e. beginning of ventricular diastole. As the left ventricle empties, its pressure falls below the pressure in the aorta, aortic blood flow quickly reverses back toward the left ventricle, catching the aortic valve pocketlike cusps and is stopped by aortic (outlet) valve closure. Similarly, as the pressure in the right ventricle falls below the pressure in the pulmonary artery, the pulmonary (outlet) valve closes. The S2 sound results from reverberation within the blood associated with the sudden block of flow reversal.
Splitting of S2 normally occurs during inspiration because the decrease in intrathoracic pressure causes more blood to be delivered to the right heart, thereby prolonging contraction and delaying closure of the pulmonic valve. A widely split S2 can be associated with several different cardiovascular conditions, including right bundle branch block and pulmonary stenosis.(wikipedia)
Assessing Lung Sound
Assessing Lung Sound

To auscultate lung sounds, move the diaphragm of your stethoscope according to the numbers on the corresponding diagram.
There are three normal breath sounds :
- (B) Bronchial Breath Sounds - loud, harsh, hight pitched
Heard over trachea, bronchi (betwen clavicles and midsternum), and over main bronchus. - (BV) Bronchovesicular Breath Sounds - blowing sounds, moderate intensity and pitch.
Heard over large airways, on either side of sternum, at the Angle of Louis, and betwen scapulae. - (V) Vesicular Breath Sounds - soft breezy quality, low pitched.
Heard over the peripheral lung area, heard at best of base lungs.
ARNP Jobs Nurse Practitioner Jobs Nurse Jobs PA jobs
NP jobs PA jobs Nurse Practitioner Jobs, Physician
Assistant jobs, Advanced Practice Jobs, ARNP jobs, Nurse Practitioner
Resumes, Nurse Jobs, Physician Jobs, CRNA jobs, Advanced Registered
Nurse Practitioner Jobs,Advanced Practice Provider,Advanced Practice
Clinician,
Nursing Care Plan | NCP Triple X Syndrome
Triple X syndrome is a condition in which a female is born with an extra X chromosome in each cell of the body. Those who have the extra chromosome in only some of their body cells are said to have triple X mosaicism.
Triple X syndrome is caused by the presence of an extra X chromosome in the cells of a female’s body. It was discovered in 1959 by Patricia Jacobs, a researcher working in a hospital in Scotland. The patient was a thirty-five-year-old woman who had undergone premature menopause. Although some girls with Triple X syndrome have learning disabilities or developmental delays, many do not. There are no unusual physical or medical disabilities associated with the syndrome; many girls with very mild symptoms may never be diagnosed. Researchers do not know why the extra copy of the X chromosome causes an increase in height and learning problems in some girls with the syndrome.
Triple X syndrome occurs in about one of every 900–1,000 girls born in the United States. It is estimated that between five and ten girls are born with the condition each day. As far as is known, the syndrome is equally common in all racial and ethnic groups. The only known risk factor for the syndrome is the mother’s age; women who are thirty-five or older when they become pregnant are at increased risk of having a daughter with Triple X syndrome.
Nursing Care Plan Signs and Symptoms
The most common cause of Triple X syndrome occurs when an egg carrying two copies of the X chromosome is involved in conception. The reason for the extra copy in the abnormal germ cell is a genetic error called nondisjunction. Nondisjunction is a random event and is not caused by anything either of the baby’s parents did or by any medications they may have taken.
During the normal process of germ cell formation, the paired chromosomes in the cell divide so that each daughter cell has only one member of the pair. In nondisjunction, one daughter cell gets both members of the chromosome pair and the other cell has none. If a germ cell carrying two copies of the X chromosome is fertilized by a normal germ cell from the other parent, the child will have three copies of the X chromosome. This genetic error is called a full trisomy X. Some girls affected by triple X syndrome children have some body cells with the extra copy of the X chromosome and some body cells without the extra copy. This condition is called mosaic trisomy X. About half of women with Triple X syndrome have the full trisomy X and the other half have mosaic trisomy X. Not all girls born with triple X syndrome have noticeable symptoms of the condition, which is why they may not be diagnosed for some years. In addition, girls with the normal number of X chromosomes may also have these features that are symptomatic of triple X syndrome:
• Slightly lower weight at birth
• Taller than other girls and women in the family
• Less coordinated; somewhat higher risk of developing back problems
• Development of language skills may be slowed
• Less assertive and quieter than most girls
• Increased risk of depression
• Intelligence that may be slightly lower than that of other girls and women in the patient’s family (Mental retardation is unusual.)
Girls with trisomy X go through puberty at the same age as girls with two X chromosomes and develop all the normal sexual characteristics of adult women. They are able to marry and have children, and do not need hormone treatments in order to become sexually mature. It is not yet known whether adult women with Triple X syndrome undergo menopause at an earlier age than most women because the condition has not been studied long enough for researchers to follow a significant number of subjects through adult life into menopause.
Nursing Care Plan Diagnosis
Triple X syndrome may never be diagnosed if the girl has no obvious symptoms. It can, however, be detected by amniocentesis before birth. Amniocentesis is a procedure in which the doctor withdraws a small amount of fluid from the sac that surrounds the baby in the mother’s uterus and examines cells from the baby’s tissues for genetic abnormalities. Triple X syndrome is sometimes discovered after birth if the girl has developmental delays or learning difficulties and is given a genetic evaluation.
Nursing Care Plan Treatment
There is no specific treatment for triple X syndrome; many doctors do not consider it a major disability. Girls with the syndrome who do have learning disabilities or emotional problems are given the same types of therapy as other children with the same conditions. An individualized treatment plan can be drawn up with the help of the girl’s doctor and teachers.
The most important aspect of treatment for the syndrome is love and support from the patient’s family. According to a Danish researcher who started one of the first triple X support groups in the world, “If conditions at home are good, stable and stimulating…learning problems rarely have any serious consequences. However, most triple X girls need remedial teaching at school at one time or another, and it is important that they get this help if and when they need it.”
Prognosis
The prognosis for girls with Triple X syndrome is generally good, particularly if their parents are loving and supportive. They are not at increased risk of other diseases as far as is known and have a normal life expectancy. They are less likely to complete college than other girls, but
almost all can finish high school with speech therapy or other additional help.While a few girls with triple X syndrome have some social difficulties, most are able to join the workforce, marry, and start families in adult life.
Nursing Care Plan Prevention
Because triple X syndrome is thought to be caused by a spontaneous genetic mutation rather than an inherited genetic defect, there is no way to prevent it.
The Future
It is possible that the increasing numbers of women having children in their thirties or forties will lead to an increase in the number of girls born with triple X syndrome. Little research has been done on triple X syndrome considering the numbers of girls affected by it; however, the conference hosted by the University of California, Davis, in 2006 offered some possible new directions. Papers were presented on the treatment of language difficulties, depression, anxiety, and developmental differences in girls with Triple X syndrome. Another presenter discussed the use of medications as part of treatment plans for these girls.
Subscribe to:
Posts (Atom)