CLIENT ASSESSMENT DATA BASE
Circulation
Persistent increase in BP over pregravid or first-trimester baseline readings after 20 wk of pregnancy (systolic elevation
> 30 mm Hg, diastolic elevation > 15 mm Hg or a BP
> 140/90 mm Hg on two consecutive readings assessed at least 6 hr apart).
History of chronic hypertension.
Jugular venous distension.
Gallop rhythm may be present.
Pulse may be decreased.
May have spontaneous bruising, prolonged bleeding, or epistaxis (thrombocytopenia).
Elimination
Oliguria/anuria may be present.
Hematuria may be noted.
Food/Fluid
Nausea/vomiting.
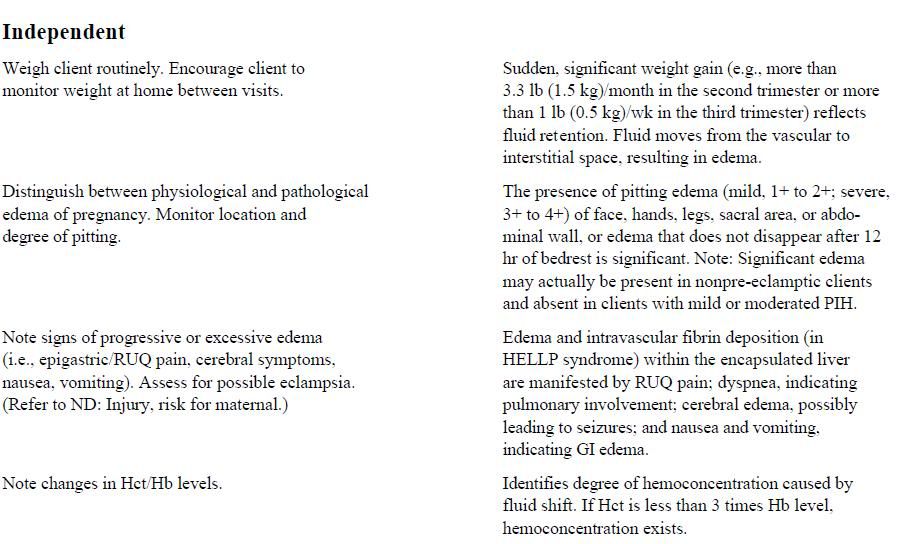
Weight gain of 2+ lb in 1 wk, 4 lb or more per month (depending on length of gestation).
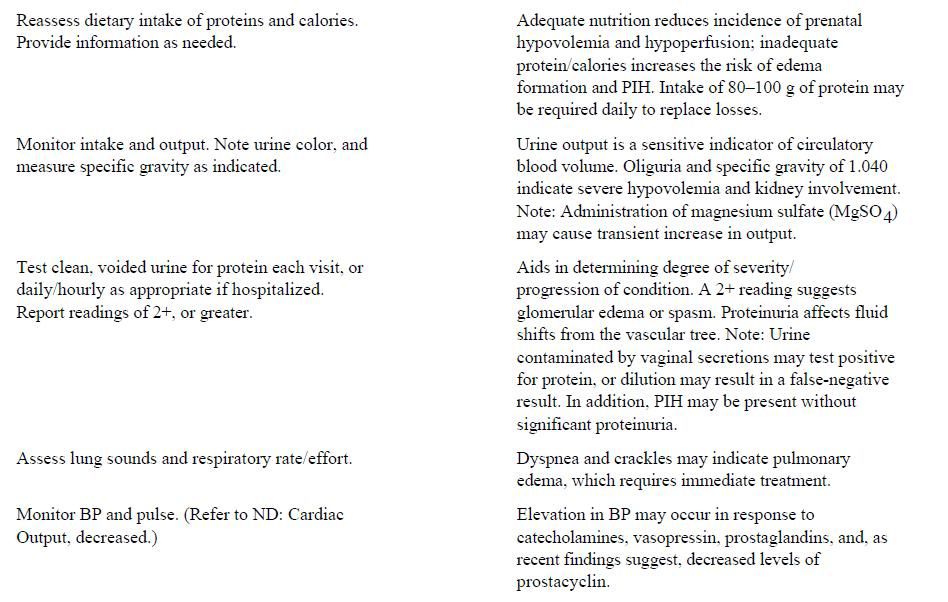
Malnourished (overweight or underweight by 20% or greater); poor protein/caloric intake.
Edema may be present, ranging from mild to severe/generalized; and may involve facies, extremities, and organ systems
(i.e., liver, brain).
Glycosuria (diabetes mellitus).
Neurosensory
Dizziness, frontal headaches.
Decreased responsiveness/somnolence.
Diplopia, blurred vision, or even loss of visual fields; scotomata (spots before eyes).
Hyperreflexia; clonus.
Convulsions—tonic, then tonic-clonic phases, followed by a period of loss of consciousness.
Funduscopic examination may reveal edema or vascular spasm.
Pain/Discomfort
Epigastric pain (right upper quadrant [RUQ] region)
Respiration
Respirations may be less than 14/min.
Safety
Rh incompatibility may be present.
Sexuality
Primigravida, multiple gestation, hydramnios, gestational trophoblastic disease (e.g.,: hydatidiform mole), hydrops
fetalis (Rh antigen-antibody)
Fetal movement may be diminished
Signs of abruptio placentae may be present (e.g., uterine tetany, tenderness)
Teaching/Learning
Adolescent (under age 15 yr) and older primigravida (age 35 yr or older) are at greatest risk
Family history of pregnancy-induced hypertension (PIH)
DIAGNOSTIC STUDIES
Supine Pressor Test (“rollover test”): May be used to screen for clients at risk for PIH, 28–32 wk gestation, although accuracy is questionable; an increase of 20–30 mm Hg in systolic pressure or 15–20 mm Hg in diastolic pressure indicates a positive test.
Mean Arterial Pressure (MAP): 90 mm Hg at second trimester indicates PIH.
Hematocrit (Hct): Elevated with fluid shifts, or decreased in HELLP syndrome (hemolysis, elevated liver enzymes, low platelet count).
Hemoglobin (Hb): Low when hemolysis occurs (HELLP syndrome).
Peripheral Smear: Distended blood cells or schistocytes in HELLP syndrome or intravascular hemolysis.
Serum Platelet Counts: Less than 100,000/mm3 in disseminated intravascular coagulation (DIC) or in HELLP syndrome, because platelets adhere to collagen released from damaged blood vessels.
Serum Creatinine Level: Elevated above 1.0 mg/dL and blood urea nitrogen (BUN): Greater than 10 mg/dL reflects severe renal involvement.
AST, LDH, and Serum Bilirubin Levels (indirect particularly): Elevated in HELLP syndrome with liver involvement.
Uric Acid Level: Greater than 5 mg/100 mL. Helpful in distinguishing preeclampsia from uncomplicated chronic hypertension.
Prothrombin time (PT), Partial Thromboplastin Time (PTT), Clotting Time: Prolonged; fibronogen decreased, FSP and FDP positive when coagulopathy occurs (DIC).
Urine-Specific Gravity: Elevated, reflecting fluid shifts/vascular dehydration.
Proteinuria: By dipstick, may be 1+ to 2+ (moderate), 3+ to 4+ (severe), or greater than 500 mg/dL in 24 h.
Creatinine Clearance: Decreased in preeclampsia (before serum BUN/Creatinine elevated).
Urinary/Plasma Estriol Levels: Decline indicates reduced placental functioning. (Estroils are not as useful a predictor as biophysical profile [BPP] because of the lag time between fetal problem and test results.)
Human Placental Lactogen Levels: Less than 4 mEq/ml suggests abnormal placental functioning (not frequently done in PIH screening).
Ultrasonography: At 20–26 weeks’ gestation and repeated 6–10 wk later, establishes gestational age and detects IUGR.
Tests of Amniotic Fluid (lecithin sphingomyelin [L/S] ratio, phosphalidylglycerol (PG), saturated phosphatidylcholine levels): Determine fetal lung maturity.
Biophysical Profile (BPP) (amniotic fluid volume, fetal tone, fetal breathing movements [FMB], fetal movements, and fetal heart rate [FHR] reactivity)/Nonstress Test (NST): Determines fetal risk/well-being.
CST: Assesses the response of the fetus to the stress of uterine contractions. Bibasilar crackles may be present. Dyspnea.
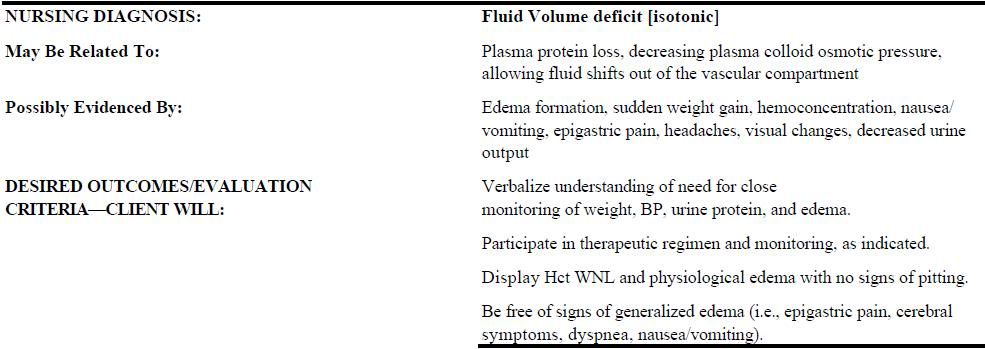
Nursing Care Plan Nursing Priorities
1. Monitor maternal, fetal, and placental status.
2. Prevent or reduce progressive fluid accumulation and other complications.
3. Promote positive maternal/fetal outcome.
4. Provide information to enhance self-care and therapeutic management.
Nursing care plan discharge goals
(Inpatient care generally not required, unless fetal compromise or eclampsia develops, or when labor process begins.)
If hospitalized:
1. Hemodynamically stable, free-of-seizure activity
2. Fetus active and in no distress
3. Condition, prognosis, therapeutic regimen understood
4. Participating in care with plan in place for home monitoring/management
No comments:
Post a Comment